After a brief foray into the uncomfortable position of being publicly humiliated, the American Board of Internal Medicine is now telling is they have begun a “transformation” of their Maintenance of Certification program. They said they got “it” wrong.
But instead of understanding “it,” they want practicing physician to forget “it” and, instead, refocus our efforts to redefine “it.”
To begin that process, they are publishing seemingly heartfelt missives claiming they’ve been “thinking a lot … about the values that we physicians share.” Even after squandering any semblance of trust by their inexcusable financial behaviors, they pretend to understand how practicing physicians feel and claim “we are united in our passion to do right by our patients and our commitment to lifelong learning.”


Top 7 Modern AI-Powered EAP Providers for Global Workforces in 2026
Discover the top AI-powered EAP providers for 2026. Compare platforms like Kyan Health and Spring Health on triage speed, global reach, and clinical quality to transform workforce wellbeing.
This is a straw dog.
They have taken accountability for the most trivial component of what they did to the practicing physician community – as if they hired damage-control consultants. Instead of coming clean, we now see they have begun a campaign to groom vulnerable physicians into believing their storyline so their largess can continue unabated.
For who is more vulnerable than a junior practicing US physicians saddled with huge educational debt? Who is more vulnerable than the junior physician trying to find a job as an employee in a large health care system hell bent on cutting costs? Who is more vulnerable than the majority of physicians who have lost their independent practices and now are placed in the ethically impossible position of serving two masters: their patients or their employers that insist they do more with less?
Like a perpetrator trying to identify areas of psychological weakness in the vulnerable practicing physicians, they continue to attempt to position themselves as our savior, rescuer, and someone who holds us in the highest regard.


Inside an Automated Healthcare Practice: Redesigning Care Around People, Not Paperwork
By reducing administrative burden and redesigning workflows around human needs, it creates space for what matters most: connection between clinicians and patients.
Trust between physicians is critically important. We rely on our colleagues in matters of life and death every day.
Actively practicing physicians cannot tolerate faux trust or press-release trust. But the members of the ABIM wouldn’t know about that. They sit on their insulated perches forcing their colleagues to pay into their flawed system first every ten years and now every two. They have assembled a rich war chest of cash assembled on the backs of their practicing colleagues and then proceed to self-select their finest sycophants to join their merry band of highly-paid regulators. And remarkably, we now find that their unproven pay-to-play scheme uses the federal government as imprimatur.
But we should understand that this loss of trust goes much further. Every professional organization that sides with the ABIM in support of the MOC program is also violating their own membership’s trust of collegiality, professionalism, and support.
Nowhere was there a better example of the pathologic nature of the siding with the ABIM than that demonstrated by a recent letter from the American College of Physician’s Executive Vice President and CEO, Steven Weinberger, MD, to their membership in response to the ABIM’s “We Got It Wrong” admission. Almost unbelievably, rather than acknowledging the realities of the ABIM’s actions, Weinberger’s letter openly threatens their membership with veiled threats of potential consequences of non-complicance with the ABIM MOC program if they choose an alternate certification pathway:
As many of you know, there has been a movement by some physicians to establish a pathway for “certification” that is independent of either ABIM or the American Board of Medical Specialties (ABMS, the umbrella organization over all specialty boards, including ABIM). We have been asked by a number of our members about “alternative pathways,” and I wanted to outline a series of questions that anyone must consider when assessing alternative options: Will an alternative pathway be credible to substitute as a credentialing requirement for hospitals and health plans? (For example, a requirement of 50 hours of CME credit over 2 years is a very low bar, in fact representing only half of the CME requirement for medical licensure in most states.)
- If you are named in a medical liability lawsuit, how will it appear when it is noted that you have not recertified through ABIM but have instead tried to show that you are “certified” through a process that has not been widely accepted and whose requirements are minimal?
- If you have a time-limited certificate from ABIM, are you willing to forfeit that primary certification in internal medicine and/or a subspecialty of internal medicine when that certificate expires? Recognize that, after your current certificate expires, not participating in ABIM’s MOC program means more than just being listed as “not participating in MOC.” It means that you are no longer certified, i.e. your initial certification is no longer valid.
- Is the fee for an alternative pathway reasonable considering both what you are getting as well as the expenses of the group that has developed the alternative pathway? For example, a fee of $169 every 2 years is almost half of the ABIM’s internal medicine MOC fee, but the alternative organization has no program or product development costs, as all it is doing is sending an electronic certificate (there is an additional charge for a paper certificate).
(Update: See the NBPAS.org’s response to the ACP)
And as if this were not bad enough, the ABIM Foundation continues to use Christine Cassel, MD, former President and CEO of the ABIM, as their spokesperson on matters of waste in our health care system in their highly-produced videos to the public when they themselves have squandered millions.
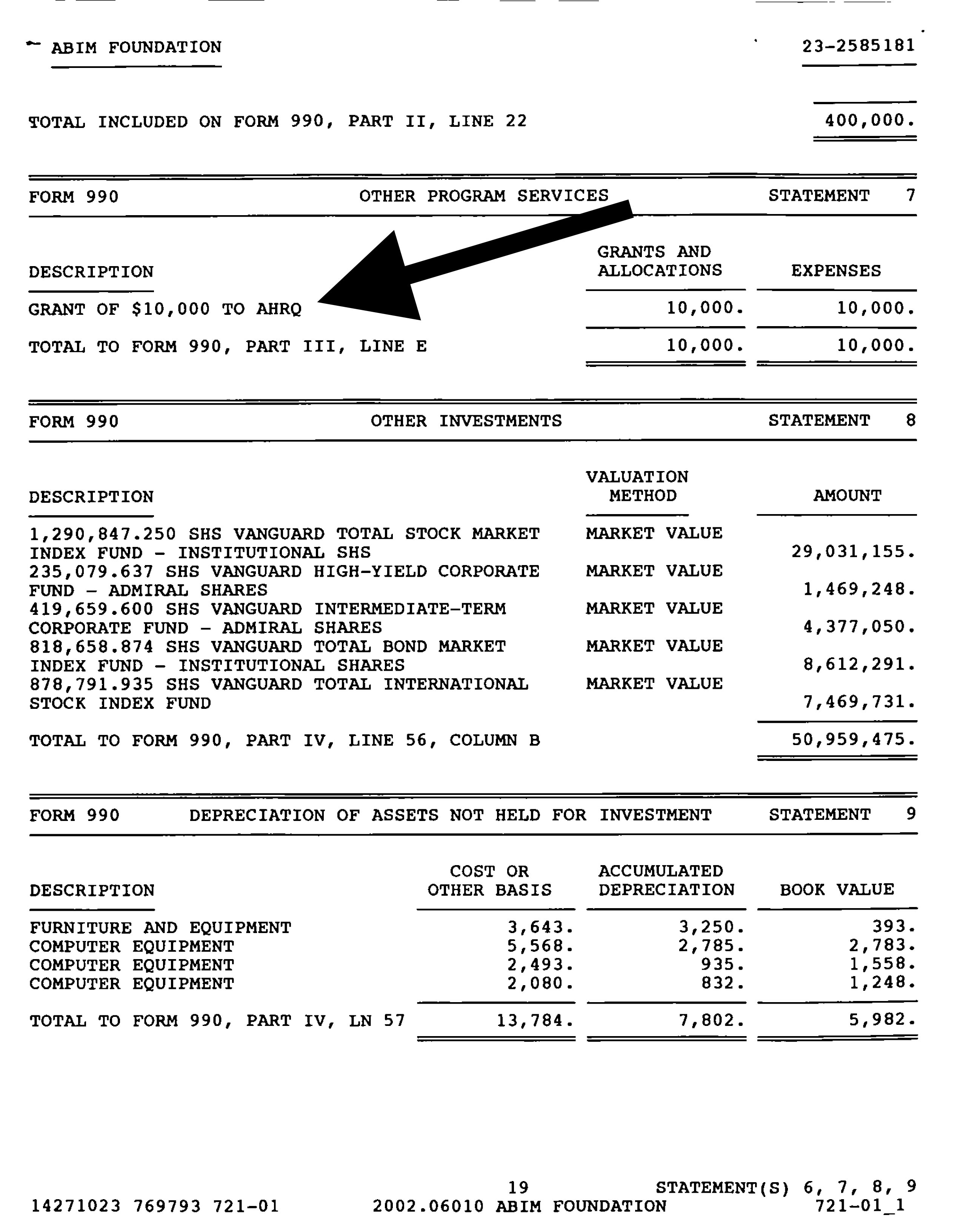
The ABIM Foundation never mentions they used coerced physician testing fees to fund their Choosing Wisely Campaign and to purchase lavish condominiums for themselves. They never disclose (and have no future plans to disclose) their many years of conflicts of interests with consulting groups, think tanks, hospital groups and little sweetheart government agency grants with practicing physicians or the public. They see no problem squandering $3.3 million dollars of physician testing fees on a contrived promise of psychometric testing techniques to add value their system. They see no problem collecting and circulating practice and meaningless survey data to their many corporate affiliates.
{kind=link}
And worst of all, they have no plans to examine their sister organization’s practice of failing as many as 22% of their test takers without ever evaluating the impact of their actions on a physician’s ability to practice or the impact such an action has on the doctors’ patients.
The ABIM and their professional society supporters have irrevocably lost the trust of America’s practicing physician community. They can’t just “groom” this away hoping for its preservation or offer threats in the MOC program’s defense. What’s done is done.
The question now becomes, can they and their many supporters ever earn it back?
Related: (registration required) “Physicians are Outraged Despite ABIM Apology for MOC Mess” Medscape – Note: 237 332 comments and growing.
Westby G. Fisher, MD, FACC is a board certified internist, cardiologist, and cardiac electrophysiologist (doctor specializing in heart rhythm disorders) practicing at NorthShore University HealthSystem in Evanston, IL, USA and is a Clinical Associate Professor of Medicine at University of Chicago's Pritzker School of Medicine. He entered the blog-o-sphere in November, 2005. He writes regularly at Dr. Wes. DISCLAIMER: The opinions expressed in this blog are strictly the those of the author(s) and should not be construed as the opinion(s) or policy(ies) of NorthShore University HealthSystem, nor recommendations for your care or anyone else's. Please seek professional guidance instead.
This post appears through the MedCity Influencers program. Anyone can publish their perspective on business and innovation in healthcare on MedCity News through MedCity Influencers. Click here to find out how.