
Researchers at Harvard Medical School and the Harvard T.H. Chan School of Public Health in conjunction with the Medicare Payment Advisory Commission (MedPAC) established a new measure, “Healthy Days at Home,” that attempts to quantify how well healthcare organizations keep people healthy and out of facility-based healthcare settings.
The full study, published in Healthcare presents a novel population-based outcome measure that quantifies how much time Medicare beneficiaries spent away from in-patient stays and other acute-care services that could help providers tailor quality-improvement initiatives to address the needs of specific patient populations.

The Power of One: Redefining Healthcare with an AI-Driven Unified Platform
In a landscape where complexity has long been the norm, the power of one lies not just in unification, but in intelligence and automation.
Current approaches to evaluating quality focus on episodes of care surrounding acute events. This results in a focus on conditions that are easily measured or clinical processes that are already considered appropriate – a phenomenon sometimes called “looking under the streetlight.” These quality measures usually appeal to a narrow range of stakeholders such as payers and do not hold much meaning for patients.
To improve the current approach to quality measurement, researchers from the Department of Health Policy and Management at Harvard Medical School and the Harvard T.H. Chan School of Public Health worked in conjunction with the Medicare Payment Advisory Commission (MedPAC) to evaluate how well healthcare organizations responsible for the health of populations keep people healthy and out of healthcare institutions. The measure, Healthy Days at Home (HDAH), was designed to reflect the quality of care provided and represent a health outcome of value to patients.
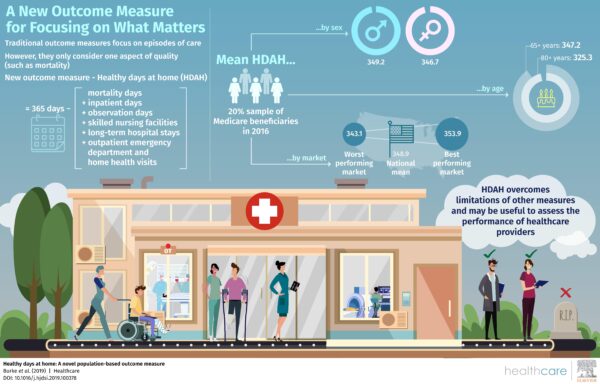
As designed, the measure represents an intimate understanding of the multidimensional nature of healthcare. HDAH is defined as the number of days spent alive and outside of institutional settings (inpatient psychiatry, ED visits, hospital stays) and analogs (home health visits). For example, a beneficiary who spent seven days in the hospital and visited the ED three times would have had 355 HDAH out of 365 calendar days. In this way, the measure captures both healthcare utilization and cost, while measuring value to patients in the form of time spent in good health.


Enhanced Direct Enrollment: Georgia Access and the Power of Partnership
Across the nation, state-based health insurance exchanges are searching for ways to better serve their communities while making enrollment easier, more personal, and more accessible for everyone.
To show how the measure could be applied, the study identified a sample of 7,817,121 Medicare beneficiaries and stratified them by those with two or more chronic conditions, three or more chronic conditions, and those aged 65 and older. The researchers sought to understand how HDAH varied across beneficiaries and across healthcare markets.
The beneficiary population was found to have a mean HDAH of 347.9. Younger beneficiaries, aged 65-68, had a mean HDAH of 347.2 compared to 325.3 for those older than 80. Those with three or more chronic conditions had an HDAH of 333.7. Lower socioeconomic status was associated with fewer HDAH due to greater mortality and higher utilization of acute and post-acute care. These results confirm our understanding of the relationship between social determinants of health and health outcomes. Other results conflicted with widely held beliefs, such as the finding that women had fewer HDAH than men, and merit further investigation.
At the market level, each additional primary care physician per 100,000 beneficiaries added 0.1 HDAH to the beneficiaries in the market. Each additional acute bed per 1,000 beneficiaries was associated with 3.7 fewer HDAH. It is important to keep in mind that while the measure displays interesting findings, they should be examined further. For example, the inverse association between hospital beds and mean HDAH could imply that a market with a lower mean HDAH may result in increased demand for acute beds, or that a greater supply of available beds is driving HDAH down.
These metrics contextualize healthcare trends that are commonly discussed but often go unquantified. For example, we could use HDAH to make the case for increased upstream intervention: the presence of chronic conditions decreased HDAH, while the number of primary care physicians per 100,000 beneficiaries increased HDAH. This is in line with current thinking that access to high-quality primary care can reduce utilization and costs in the long run, and is consistent with what patients actually want: more healthy days at home.
Common quality measures, such as mortality, are fairly blunt and do not capture less severe harms that are important to patients and their families. Utilization measures are narrowly focused and do not account for more important outcomes such as mortality or injury. Quality measures limited to acute events fail to credit providers that prevent such episodes in the first place. By comparison, HDAH encompasses mortality and utilization, while also being easy to administer across populations and markets.
HDAH has a myriad of uses. Individual organizations could measure HDAH across their patient populations and deliver healthcare in line with patient priorities. Beneficiaries may be able to use the measure to make more informed choices about how they choose to receive care. Ultimately, the HDAH measure represents a meaningful way to compare differences in outcomes across populations in a way that is easy for beneficiaries, policymakers, providers, and payers to understand.
The full article, “Healthy Days at home: A novel population-based outcome measure” written by Laura G. Burke, E. John Orav, Jie Zheng and Ashish K. Jha was published in Healthcare: The Journal of Delivery Science and Innovation and can be found on ScienceDirect.
Through a partnership with Elsevier, MedCity News will present a news article each month on a notable topic and will link to the full study that will be available for the general public for a limited period of time. The goal is to highlight important research being undertaken as the industry is undergoing a fundamental shift. The study highlighted in this article will be available until May 3.
Infographic and Photo: Elsevier and Dean Mitchell, Getty Images